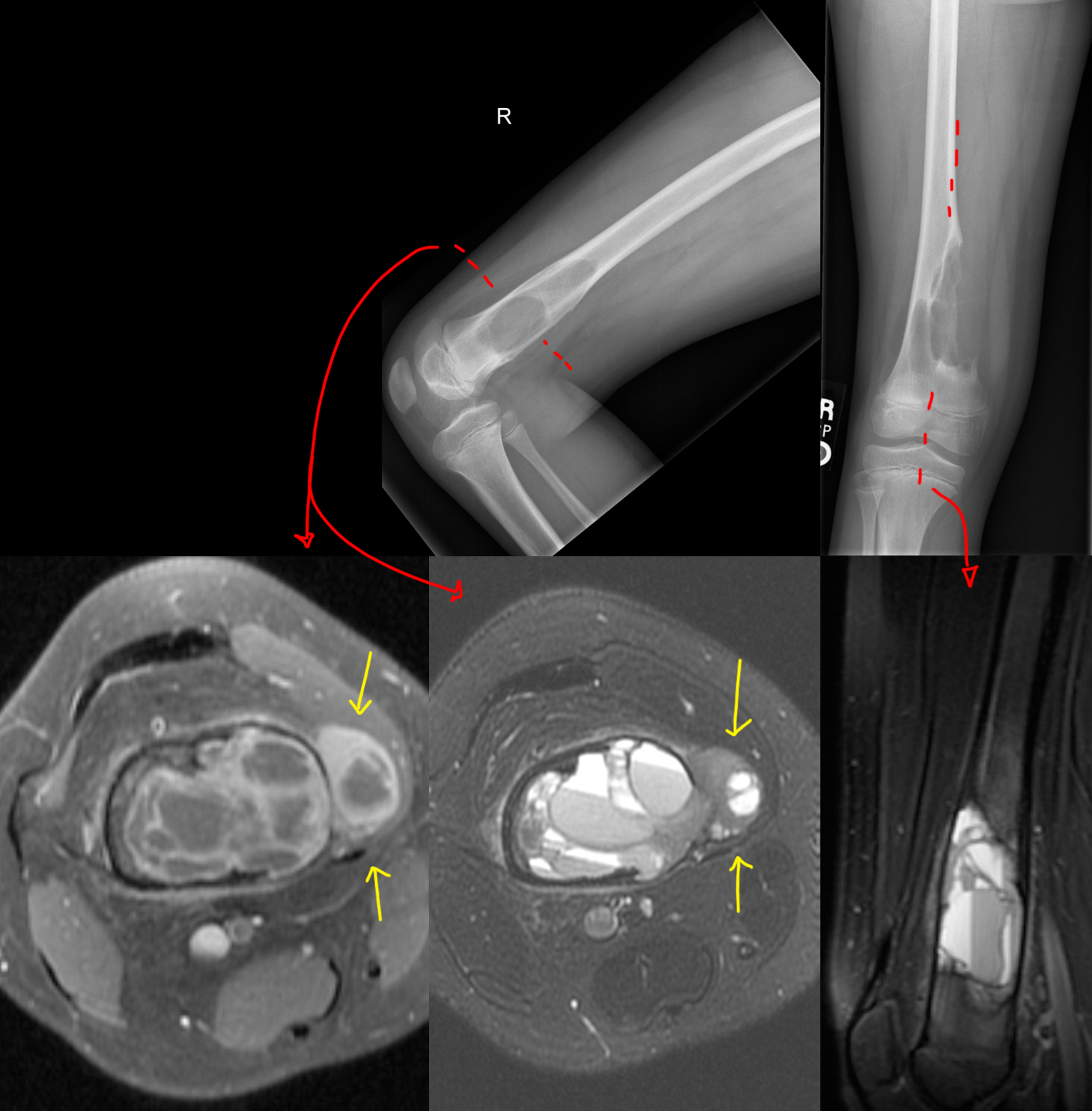
I remember this episode quite well because it happened around the time I decided to get into the medical field. In the episode, a young teacher had a first-time seizure while in the middle of teaching. House and team attempted to get a brain MRI, but she got an allergic reaction from the IV contrast. Thereafter, some drama happens, and at some point, they break into her house, find out she's been eating raw pork (wtf?), and diagnose her with the tapeworm infection associated with eating raw pork, cysticercosis (and neurocysticercosis, since it also involved her brain). They took an x-ray of her leg to show all the parasites in the muscles, and then House scolds her for being stupid. I remember thinking that was such as crazy medical story.
The reality is - they could have just repeated the brain MRI minus the contrast part, and the radiologist would have been able to identify neurocysticercosis without issue. House would have complained to Cuddy that she really was wasting his time with these basic cases, and the episode would have lasted 15 minutes tops...
Anyhow, this is a 25 year old Hispanic from jail. Just like the House episode, he presented with first time seizure and headaches.
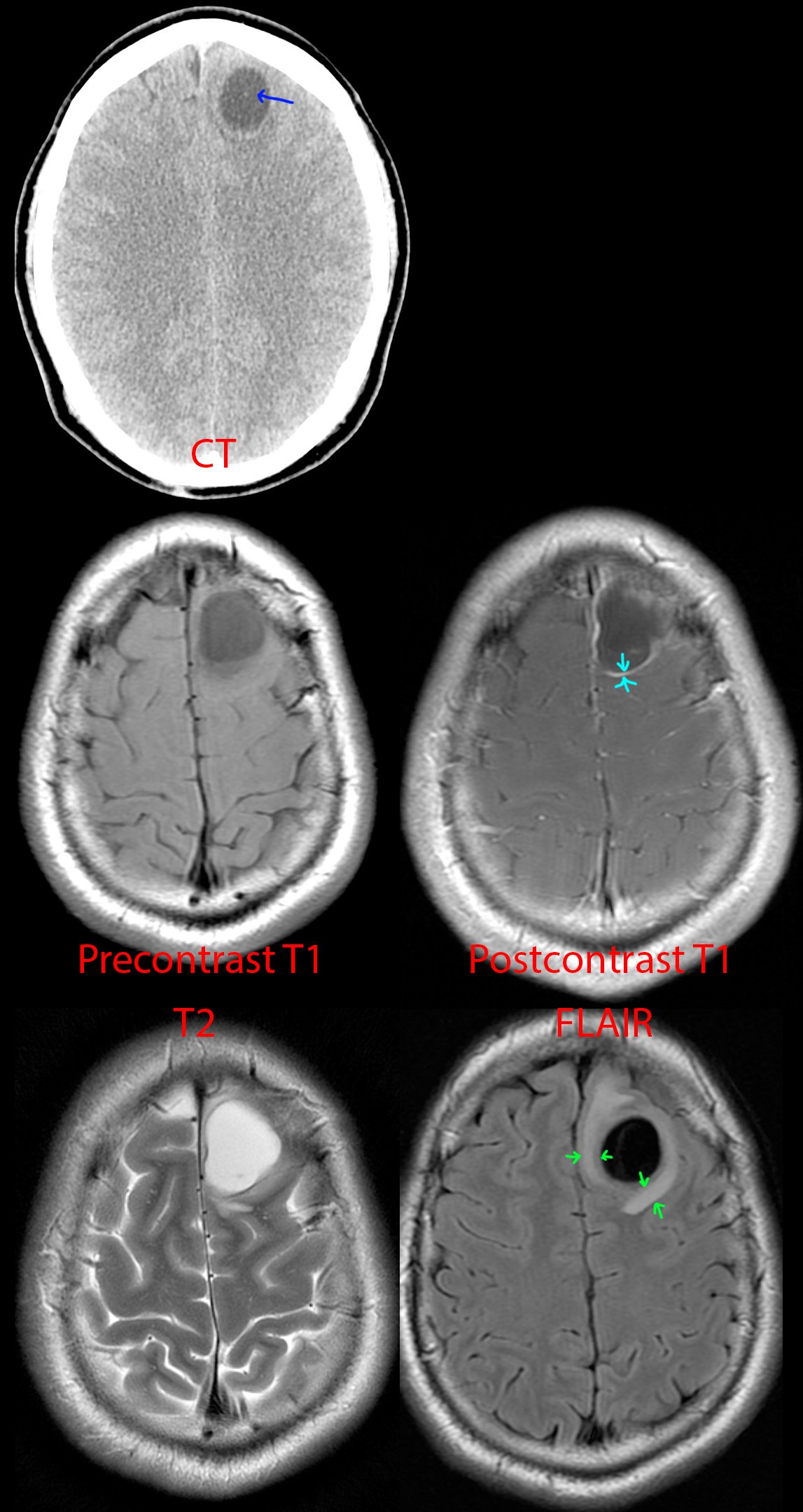
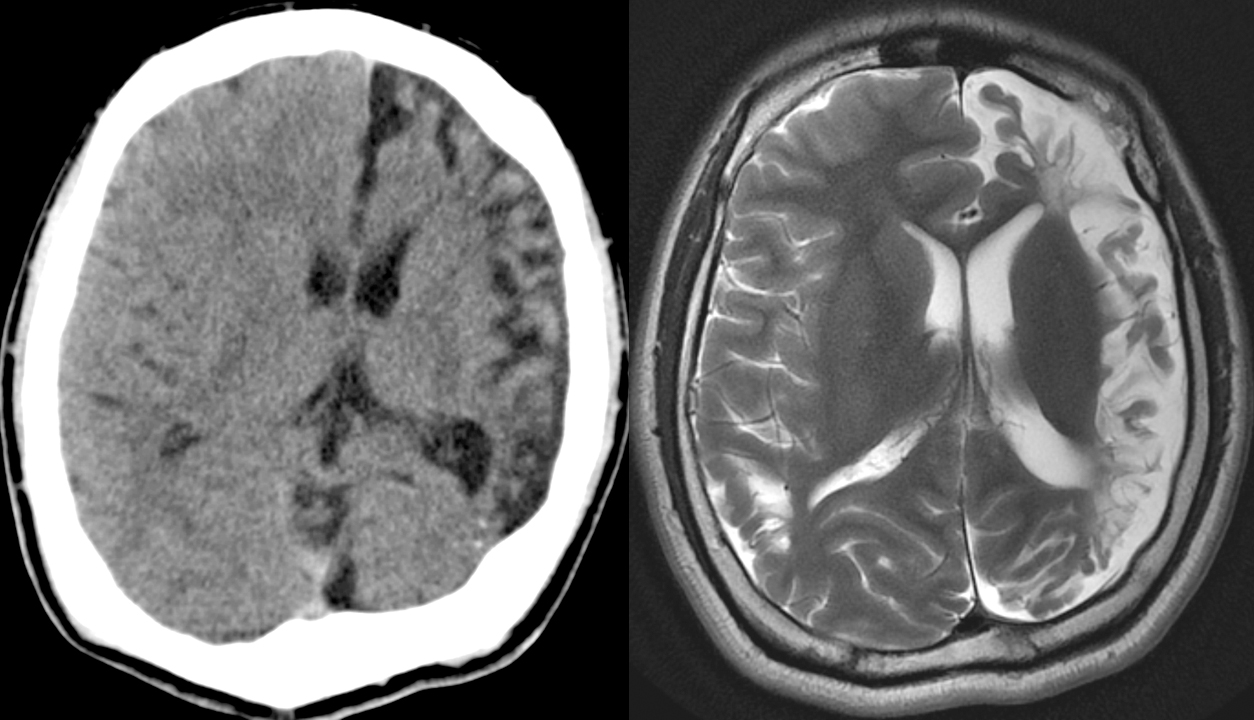
CT of the head [top] shows a cystic lesion in the left frontal lobe. If one pays attention, one can see a small dot (blue arrow) within the cyst representing the scolex of the tapeworm parasite. Just from the CT appearance, history of seizure, and risk factors of jail (the parasite thrives in areas of low sanitation) and Hispanic (the parasite is endemic to South America), neurocysticercosis is the top possibility. A differential diagnosis of cystic brain tumor is provided to complete the picture.
MR [middle and bottom] shows a cystic lesion again. After giving IV contrast [middle right], one can see the cyst has a thin wall of enhancement (teal arrows). On T2 [bottom left] and especially FLAIR [bottom right], one can see a rim of swollen brain (green arrows) from the inflammation going on around the parasite.
This was diagnosed as neurocysticercosis in the colloidal vesicular stage and antiparasite medication was started.