Radiology
594 readers
3 users here now
A community for all things related to medical imaging!
RULES:
-1. Please follow the Lemmy.World Server Rules.
-1A. Please be civil.
-1B. Please be respectful when discussing medical cases. While we do not wish to impose a somber tone upon this community, please remember that there are real patients behind the images.
-2. No patient-identifiable information. There is zero tolerance for breaching patient confidentiality laws. De-identified information is allowed under HIPAA, the US patient confidentiality law. Consent is not required when posting de-identified information.
-3. No requests for medical advice or second opinions. Please go to your physician/provider for assistance. Online strangers will never know your clinical history as well as your actual healthcare team, nor will the images posted here be of sufficient quality or completeness for diagnostic interpretation. Any content or discussions in this Community should be considered for educational purposes only, and their accuracy or quality with regards to standard of care cannot be guaranteed.
-4. No spam or advertising. Products or companies that are mentioned as a natural course of discussion are allowed.
-5. Please do not spread misinformation.
-6. Moderators have final say in their decisions. Please, no rules lawyering.
Posts:
Only moderators may post in this community pending Lemmy's implementation of a moderator-approval process. Until that happens, you may post general comments or questions in the stickied megathread. You may also request the moderators to post on your behalf via DM, pending time and availability.
founded 1 year ago
MODERATORS
1
2
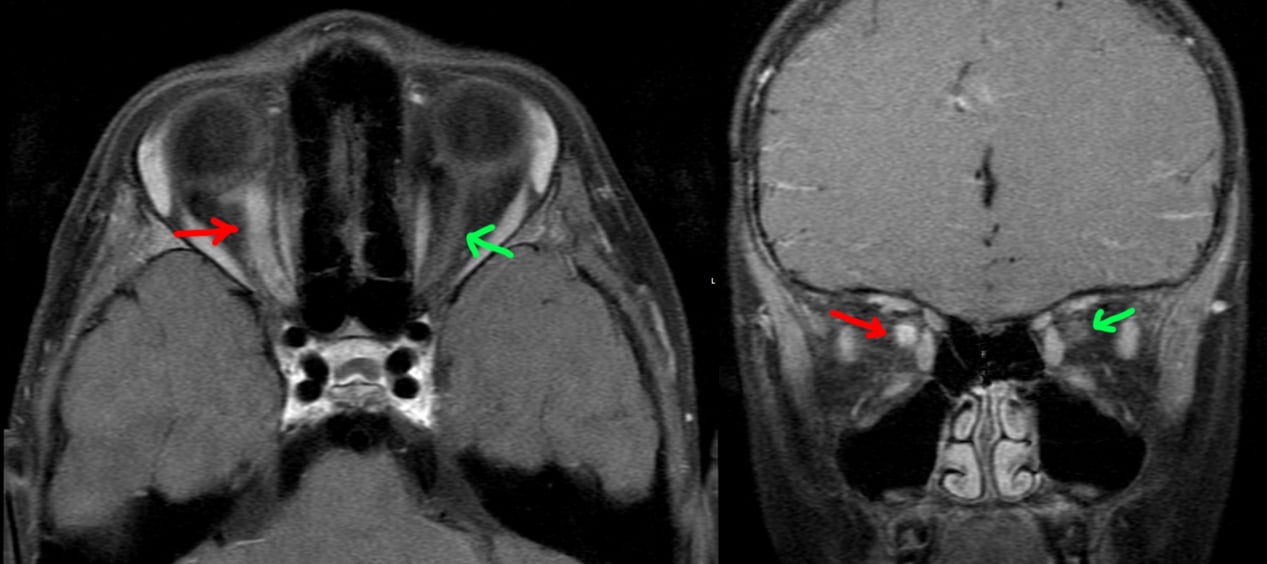
5 year old patient with 1 week of right eye blurry vision, then several days of right eye pain. Physical exam notable for right papilledema and progressively worsening vision.
MRI postcontrast through the orbits shows an enlarged, hyperenhancing right optic nerve (red arrow) compared to the normal left side (green arrow), compatible with optic neuritis.
A lumbar puncture was performed: no oligoclonal bands, no aquaporin 4 IgG, positive anti-MOG. The patient was treated with prednisone with return to normal vision a few months later.
Final diagnosis: optic neuritis from myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD).
3
This patient had episodic electric/shooting/radiating pain of the left face. An MRI was done.
[Top]: Axial heavily T2-weighted image (bright = CSF, dark = not CSF) at the level of trigeminal nerve (cranial nerve V / CN5), shows a normal right CN5 (green). The left CN5 seems to be splayed out by another tubular structure (red), which is the superior cerebellar artery (SCA).
[Bottom Left]: Sagittal reconstruction of the normal right CN5 (along the blue line).
[Bottom Right]: Sagittal reconstruction of the left CN5 shows the left SCA contacting the left CN5. The close proximity of the left SCA and its arterial pulsations likely irritate the cranial nerve, which is the primary sensory nerve of the face, causing trigeminal neuralgia.

4
1
Grynfeltt-Lesshaft hernia. (This will be the last case I post for a few days.) [Abdominal] [CT]
(lemmy.world)
Incidental finding of a superior lumbar hernia (Grynfeltt-Lesshaft hernia). In this case, only a lobule of retroperitoneal fat is herniating through the defect, but organs can also herniate through.

5
Continuing the theme of things extending into spaces they don't belong in, this is an incidental finding of an inguinal hernia that contains a small portion of the bladder. The patient got the CT for other reasons.
Bowel into inguinal hernia causing bowel obstruction.
Appendix into inguinal hernia, incidental finding.
Ventriculoperitoneal shunt into inguinal hernia, incidental finding.

6
[LEFT]: This patient had one of the longer cerebellar tonsillar herniations I've seen. The tonsil is peg-like in shape and extends quite far below the foramen magnum to the level of the C2 posterior arch. As a result, there is crowding at the foramen magnum that is enough to impede CSF flow, resulting in hydrocephalus with dilated ventricles. Partly seen in the cervical cord from C2 and below is a syrinx, an associated finding. Chiari I is thought to be due to not enough space provided for the cerebellum by the calvarium or skull base shape, causing it to herniate into the spinal canal and cause trouble.
[RIGHT]: A comparison normal from online for you to compare the cerebellar tonsils.

7
[LEFT]: The midbrain has a deep interpeduncular cistern, and the superior cerebellar peduncles are very prominent and elongated, making the brainstem at this level look like a molar tooth. This is a classic finding in Joubert syndrome.
[RIGHT]: A comparison "normal" midbrain. However, this patient's brain is not normal at all. Can you find the abnormalities?
Answer
Compare the left and right temporal lobes in [RIGHT] to the [LEFT] image. Look at how many more gyri and sulci there are in the [LEFT] image. The [RIGHT] patient has a diffuse pachygyria (abnormally reduced brain gyrations). Both Joubert syndrome and pachygyria arise from failure of neurons to migrate, although the genes involved and underlying mechanism are different between the two. (NB: Pachygyria is just a descriptive term for less than normal number of gyri, which can be from a large number of causes mostly having to do with abnormal neuron migration.)

8
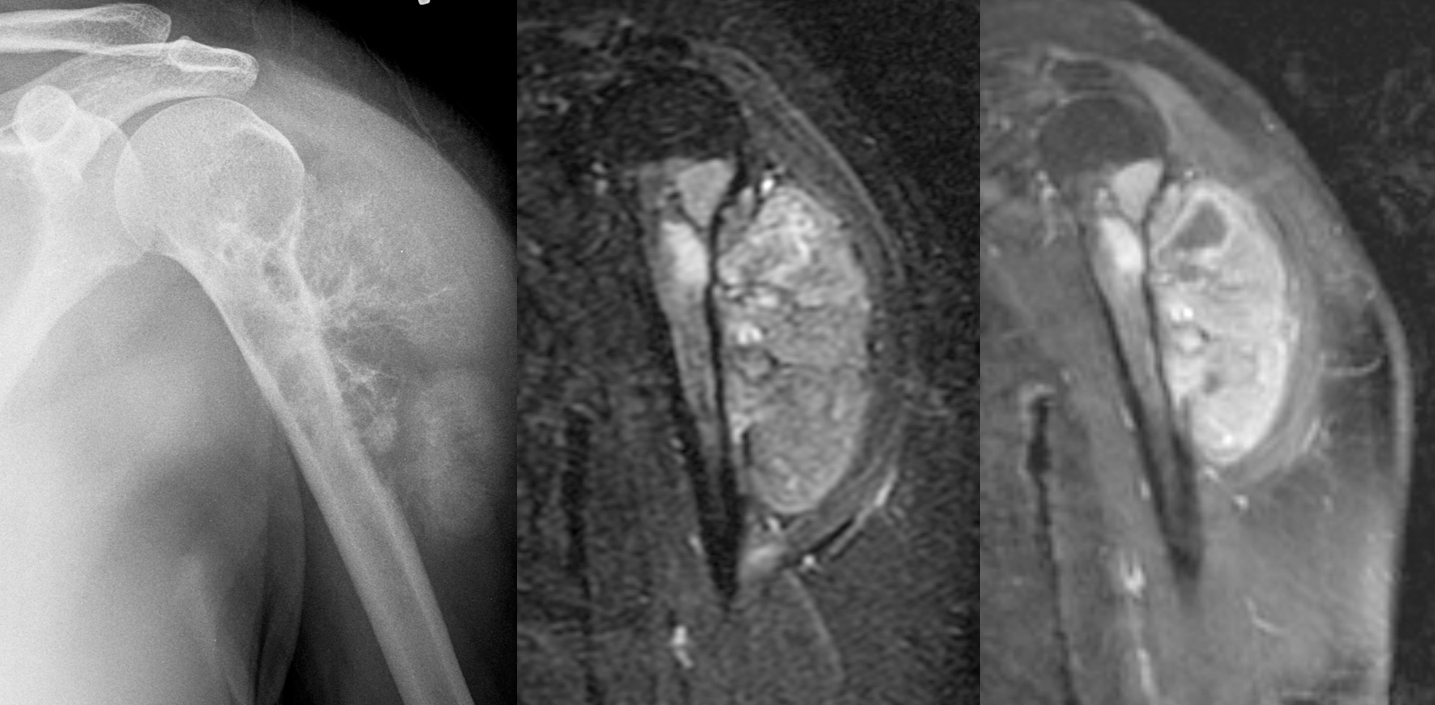
Female in her 30s with painful left shoulder.
[Left]: X-ray shows a mass arising from the left proximal humerus and extending into the adjacent shoulder soft tissues with really aggressive periosteal reaction ("hair on end"). The proximal humerus itself is also heterogeneous with lucent areas. The lateral surface of the upper humerus shows "saucerization," where the cortex is thinned out and looks like a saucer seen on edge.
[Middle]: MRI IR sequence shows a hyperintense bony mass with large soft tissue component.
[Right]: MRI postcontrast T1 IDEAL shows that the mass is enhancing.
This turned out to be high-grade surface osteosarcoma.
9
33 year old female with abdominal pain, abdominal distention, nausea/vomiting, early satiety, and weight loss.
Bottom right: Ultrasound done in a panorama shows how distended the abdomen is by a large multi-cystic mass.
Top right: Non-panoramic ultrasound image shows how limited the imaging modality is in being able to cover such a large mass. This image also shows a more solid area within the mass.
Left: CT images approximately where the ultrasound was done.
The patient underwent laparotomy with removal of the ovarian, fallopian tube, and appendix. There was a large ovarian cyst that was draining serous fluid (watery), mucinous fuid (mucus-like), and blood. The final path was as titled.

10
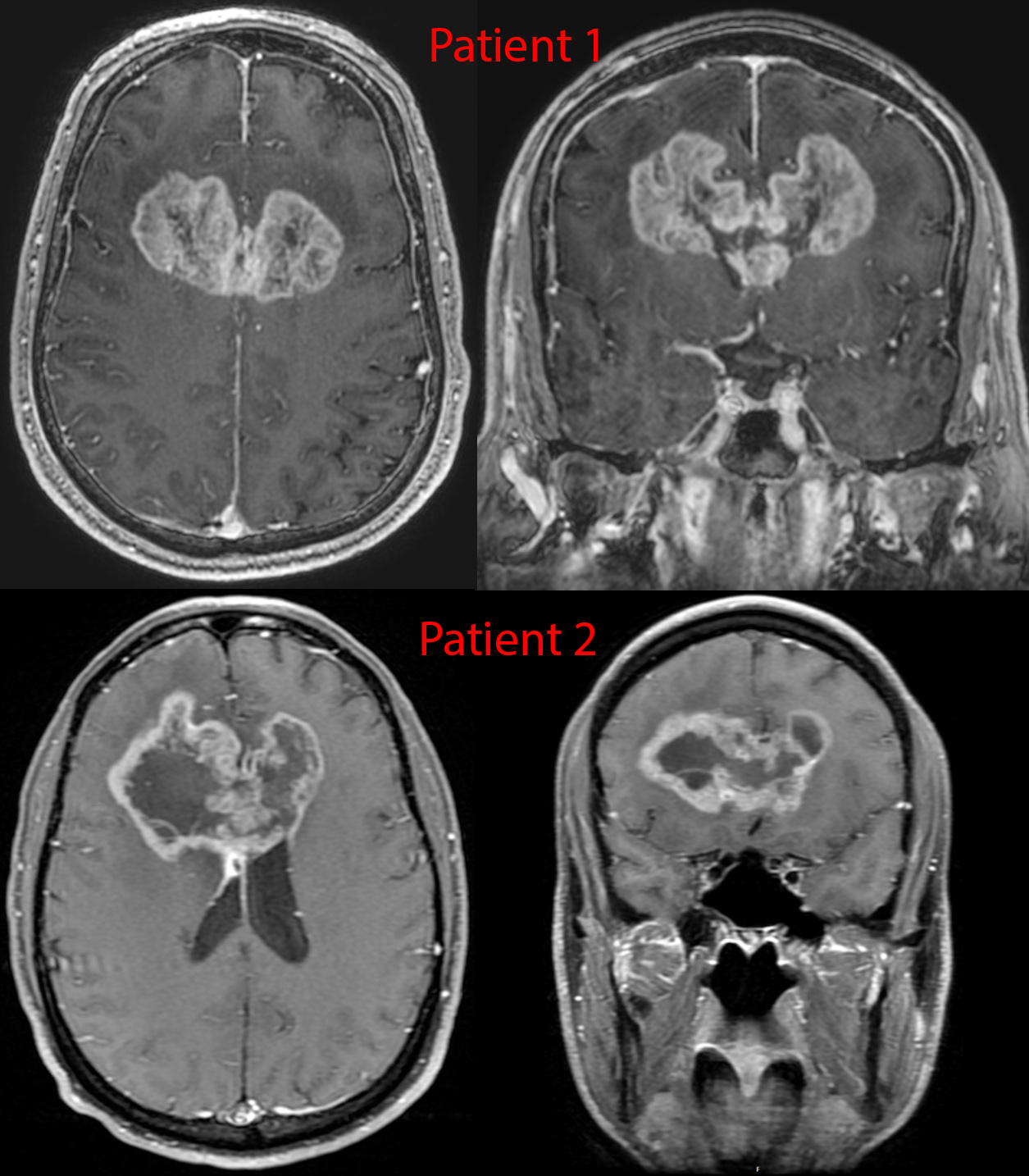
Postcontrast imaging of 2 patients with glioblastoma. These tumors are notorious for spreading along the white matter tracts - in this case the transverse fibers of the corpus callosum, given them a classic "butterfly" appearance.
11
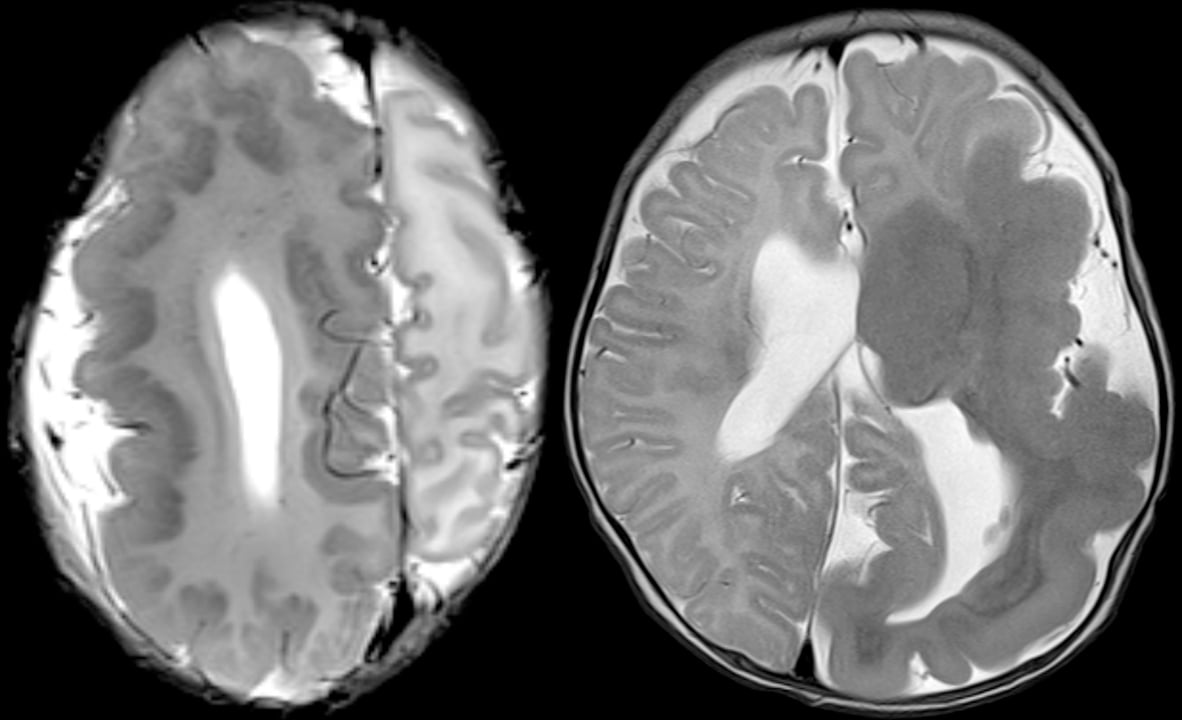
Two different patients with genetic disorders resulting in overgrowth of the brain.
These represent mutations in cell cycle and cell metabolism genes that lead to larger cells and/or more cells. These types of disorders tend to have mosaicism of some form, which is to say some cells have the mutation active while others don't. The distribution of these cells can be very geographic/regional - in these two cases, one hemisphere of the brain is involved.
Compare this against a previous case with hemispheric atrophy.
12
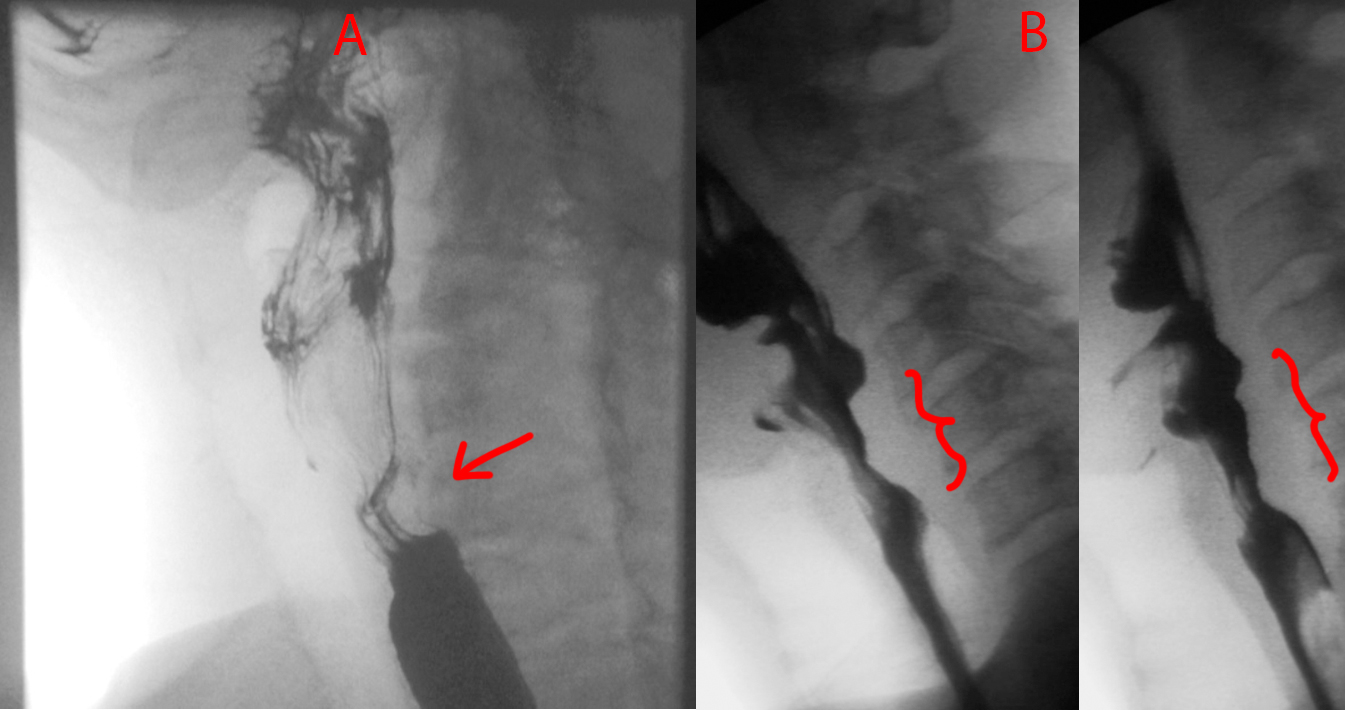
Quick one today. Take a look at Patient A and Patient B.
Patient A has a smooth focal indentation of the posterior cervical esophagus.
Patient B has a broader indentation that is also irregular and nodular along its contour.
Patient A has a cricopharyngeal bar, which is a prominence caused by the cricopharyngeus muscle that can cause dysphagia if it gets really prominent. Patient B has esophageal squamous cell carcinoma.
13
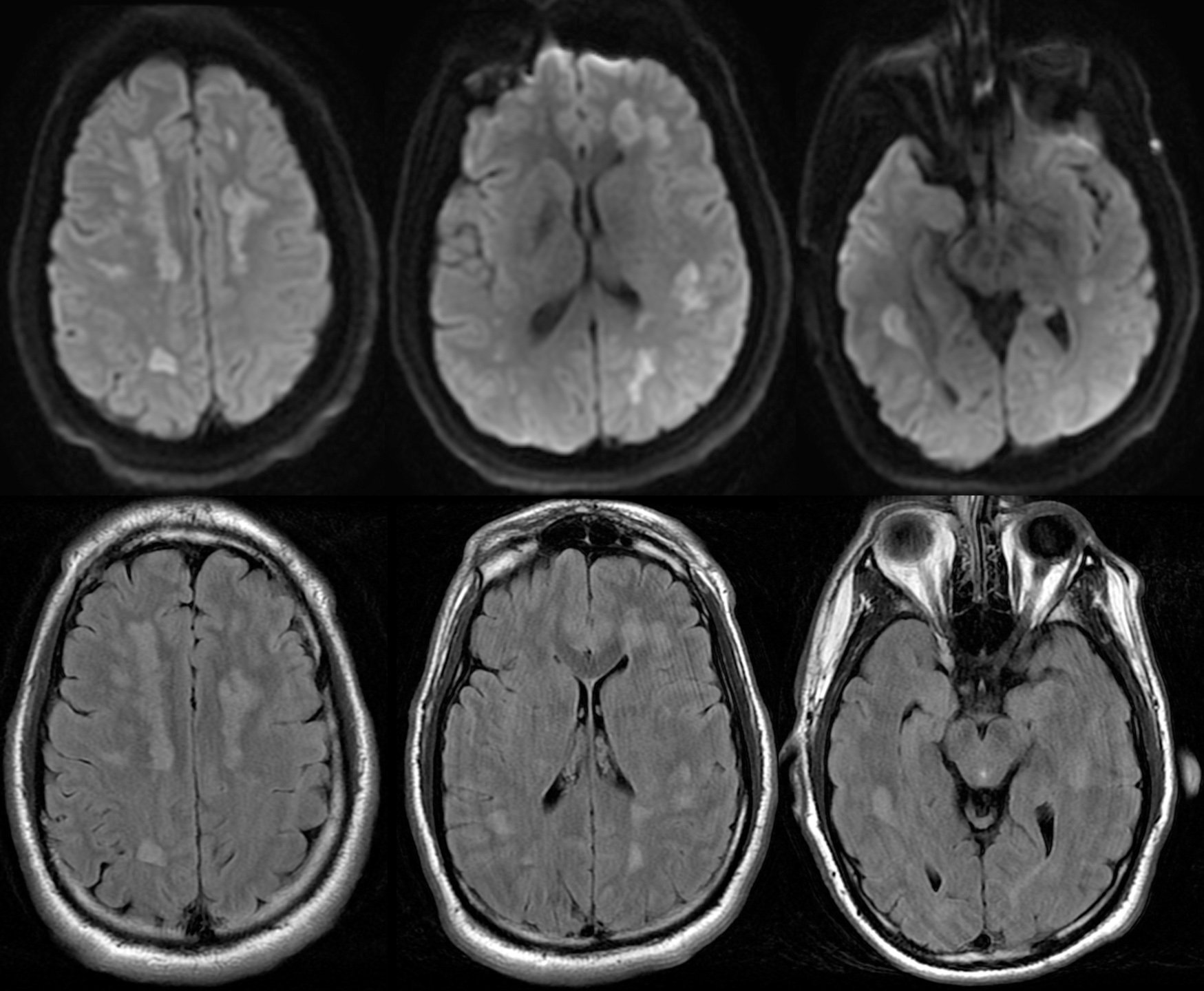
Patient was a young adult working in finance at a major tech company found to be mute and diaphoretic.
Physical exam notable for fever, tachycardiac, hypertension, awake but not following commands, aphasic, and with hyperreflexia and muscle ridigity. CK peaked to 11,344.
MRI shows multiple ovoid to splotchy confluent lesions in the white matter with diffusion restriction. Lesions also enhanced with hyperperfusion (not shown).
Urine drug test positive for cocaine. Infectious work-up was negative. Steroids were started with good recovery.
Patient denied knowingly taking cocaine but did say weekly use of what they thought was MDMA with friends...
Final diagnosis: Levamisole-induced leukoencephalopathy. Levamisole is an antiparasite medication that is no longer used in the US but still in some other countries. It is a common cutting agent in cocaine. It's neurotoxic effects primarily come from causing demyelination.
14
I remember this episode quite well because it happened around the time I decided to get into the medical field. In the episode, a young teacher had a first-time seizure while in the middle of teaching. House and team attempted to get a brain MRI, but she got an allergic reaction from the IV contrast. Thereafter, some drama happens, and at some point, they break into her house, find out she's been eating raw pork (wtf?), and diagnose her with the tapeworm infection associated with eating raw pork, cysticercosis (and neurocysticercosis, since it also involved her brain). They took an x-ray of her leg to show all the parasites in the muscles, and then House scolds her for being stupid. I remember thinking that was such as crazy medical story.
The reality is - they could have just repeated the brain MRI minus the contrast part, and the radiologist would have been able to identify neurocysticercosis without issue. House would have complained to Cuddy that she really was wasting his time with these basic cases, and the episode would have lasted 15 minutes tops...
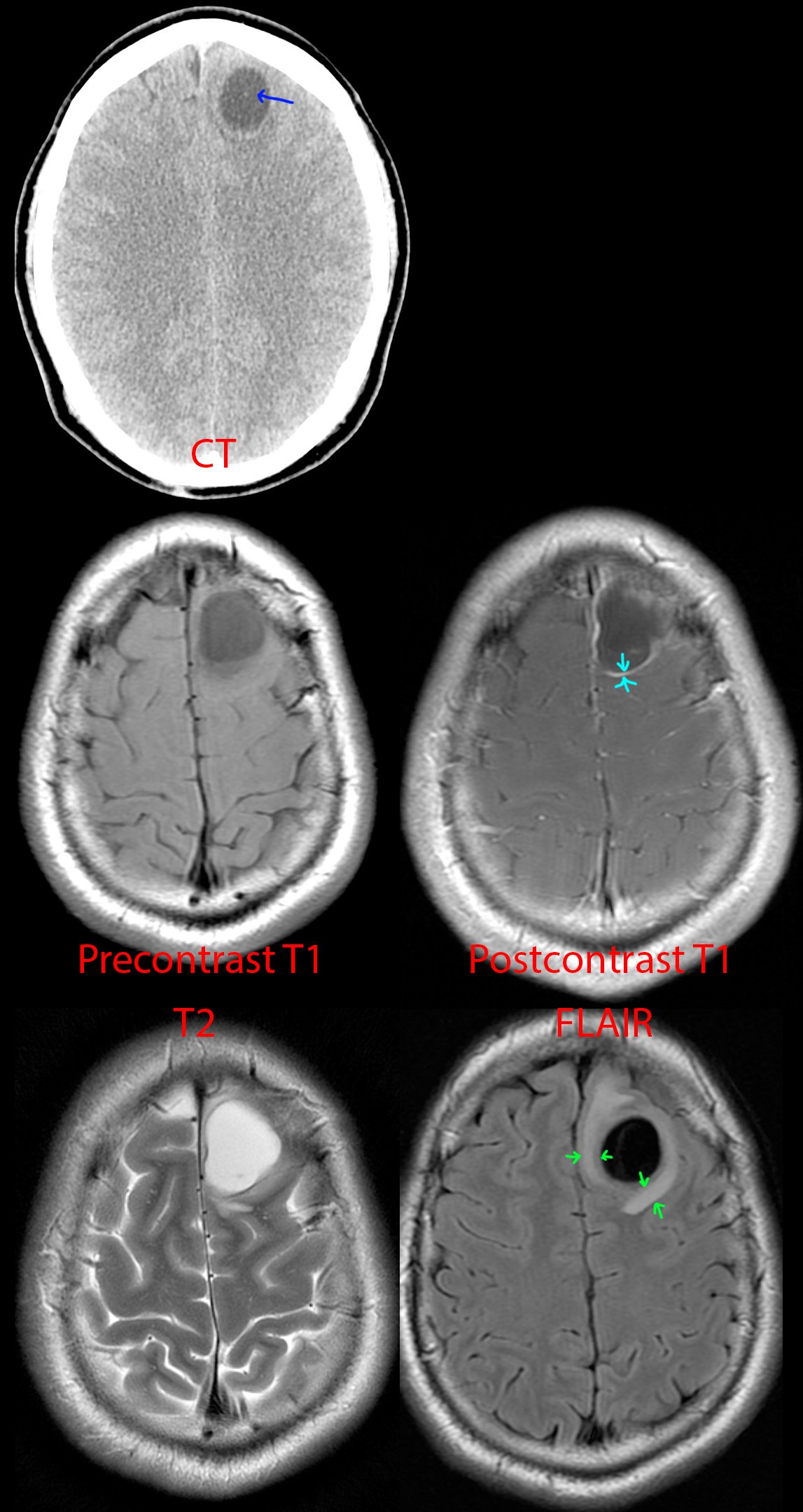
Anyhow, this is a 25 year old Hispanic from jail. Just like the House episode, he presented with first time seizure and headaches.
CT of the head [top] shows a cystic lesion in the left frontal lobe. If one pays attention, one can see a small dot (blue arrow) within the cyst representing the scolex of the tapeworm parasite. Just from the CT appearance, history of seizure, and risk factors of jail (the parasite thrives in areas of low sanitation) and Hispanic (the parasite is endemic to South America), neurocysticercosis is the top possibility. A differential diagnosis of cystic brain tumor is provided to complete the picture.
MR [middle and bottom] shows a cystic lesion again. After giving IV contrast [middle right], one can see the cyst has a thin wall of enhancement (teal arrows). On T2 [bottom left] and especially FLAIR [bottom right], one can see a rim of swollen brain (green arrows) from the inflammation going on around the parasite.
This was diagnosed as neurocysticercosis in the colloidal vesicular stage and antiparasite medication was started.
15
1
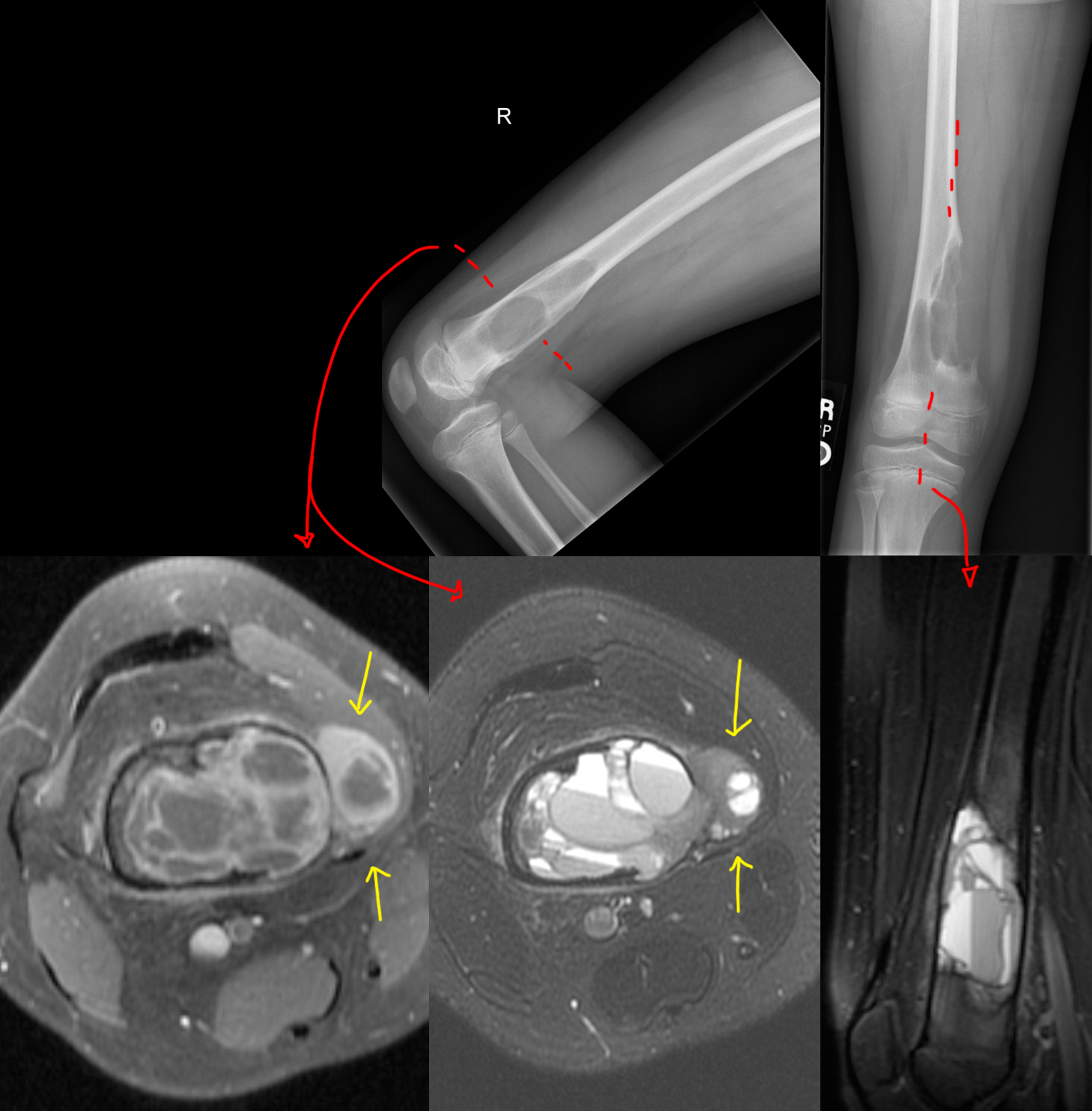
10 year old with insidious onset of right medial thigh pain. [Musculoskeletal] [XR] [MR]
(lemmy.world)
[Top]: X-ray shows a lucent, bubbly, lesion of the distal femur at the metaphysis. On the frontal view [top right], there is breakage through the medial femoral cortex into the adjacent soft tissues, not a good sign.
[Bottom]: MRI shows a multicystic lesion filling the distal femur containing multiple locules, many with fluid-fluid, fluid-debris, and fluid-hemorrhage levels. The most common lesions with this striking appearance are aneurysmal bone cyst, giant cell tumor, or telangiectatic osteosarcoma. Unfortunately, there is clearly extension of the bone tumor beyond the bone (yellow arrows), which favors a more aggressive neoplasm from that differential diagnosis - this turned out to be telangiectatic osteosarcoma.
16
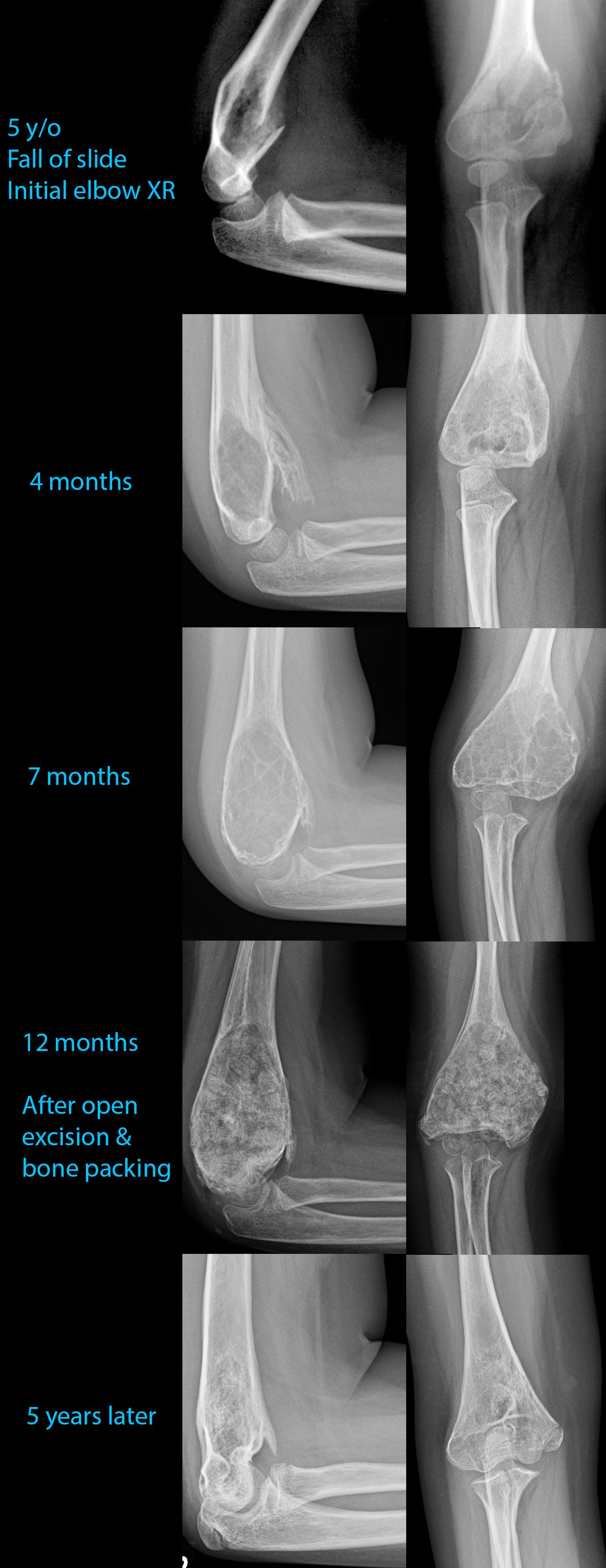
5 year old who fell off a slide.
Initial imaging shows a comminuted fracture through the distal humerus, compatible with a supracondylar fracture. Nothing else appreciable here, except maybe in retrospect some lucency of the distal humerus where the fracture is.
4- and 7-month follow-up radiographs shows a growing lucent lesion of the distal humerus, expanding the bone there. It has a multicystic appearance. A diagnosis of large simple bone cyst versus aneurysmal bone cyst was proposed.
12 month follow-up was done after the cyst was opened surgically, its contents scraped off, and the resulting cavity was packed with allograft bone chips. At surgery, this turned out to be an aneurysmal bone cyst.
5 year follow-up shows involution of the cyst cavity with some residual heterogeneity and a bone spur at the anterior aspect of the distal humerus.
17
1
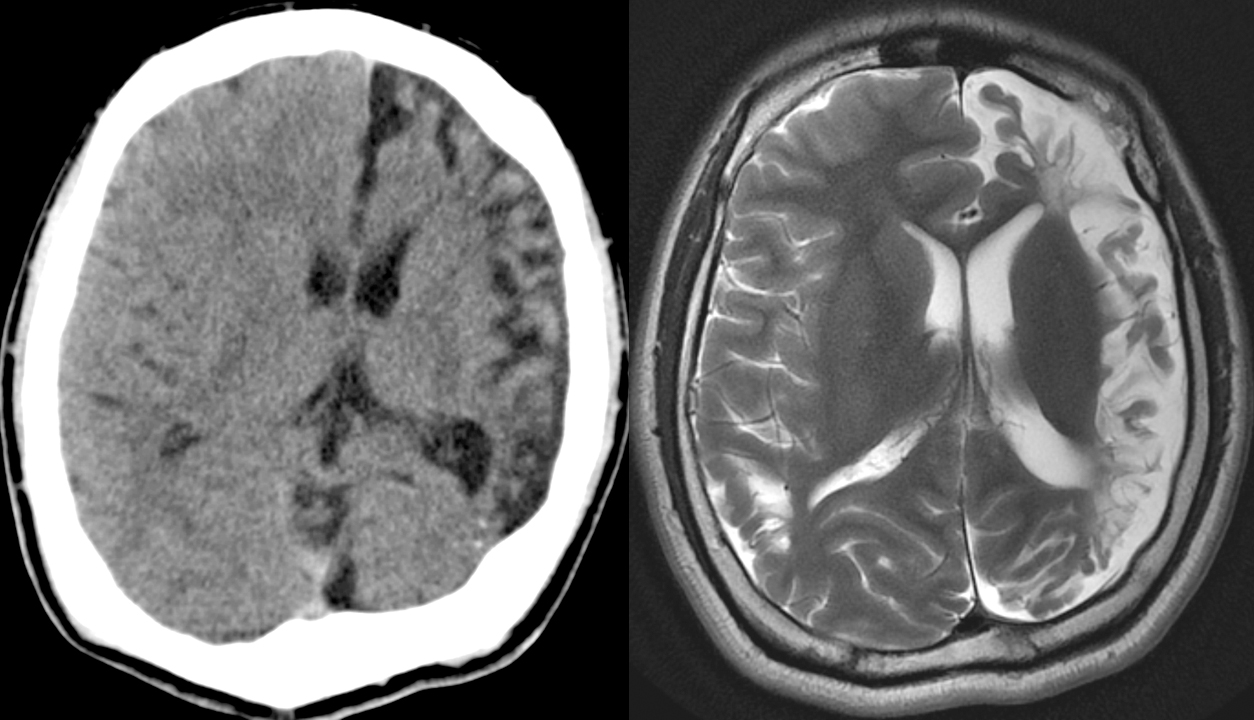
23 year old with head injury since age 2. Seizures and right hemiparesis since age 10. [Neuroradiology] [CT] [MR]
(lemmy.world)
[Left]: Head CT shows left hemispheric volume loss. The injury happened early enough that even the skull is smaller on that side.
[Right]: Brain MRI shows the severe left hemispheric atrophy. Some of the brain gyri have bulbous ends and a thin neck, resembling mushrooms, a shape called ulegyria and consequence of the brain atrophy. The left lateral ventricle is mildly enlarged due to the atrophied brain.
18
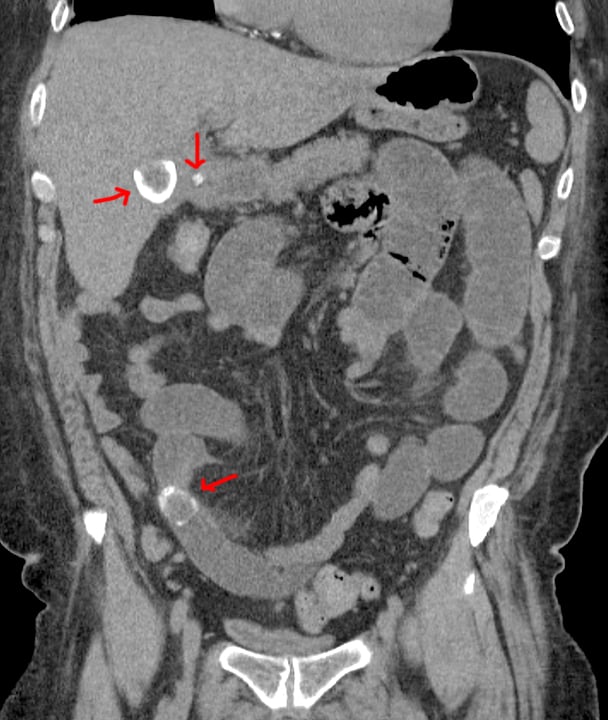
Red arrows point to 2 big gallstones, top one in the gallbladder and bottom one obstructing a small bowel loop, and a small gallstone in the cystic duct.
19
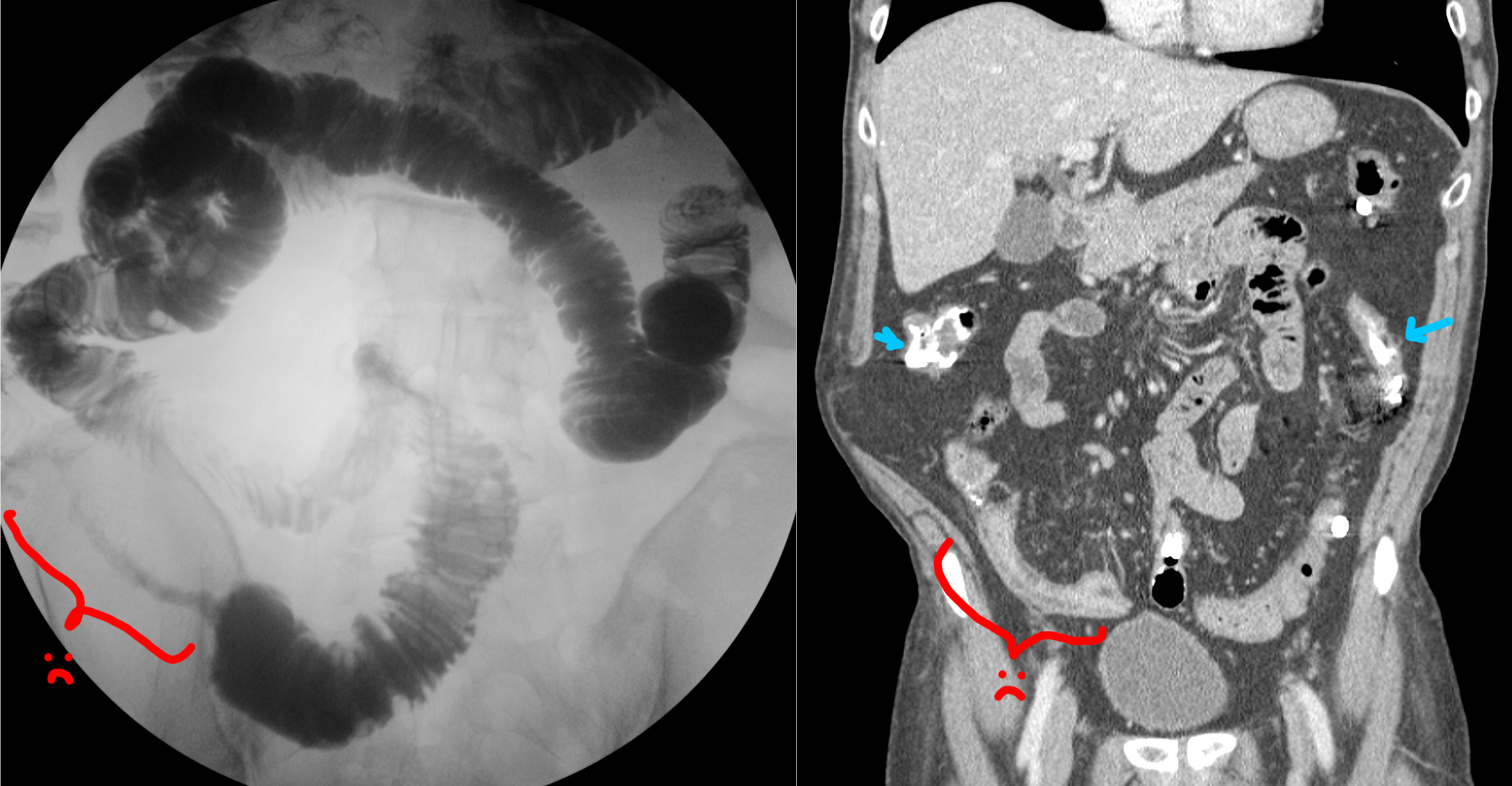
Red lines point to hernia entry. Red arrow points to where the bowel tapers and becomes obstructed as it enters the hernia sac.

20
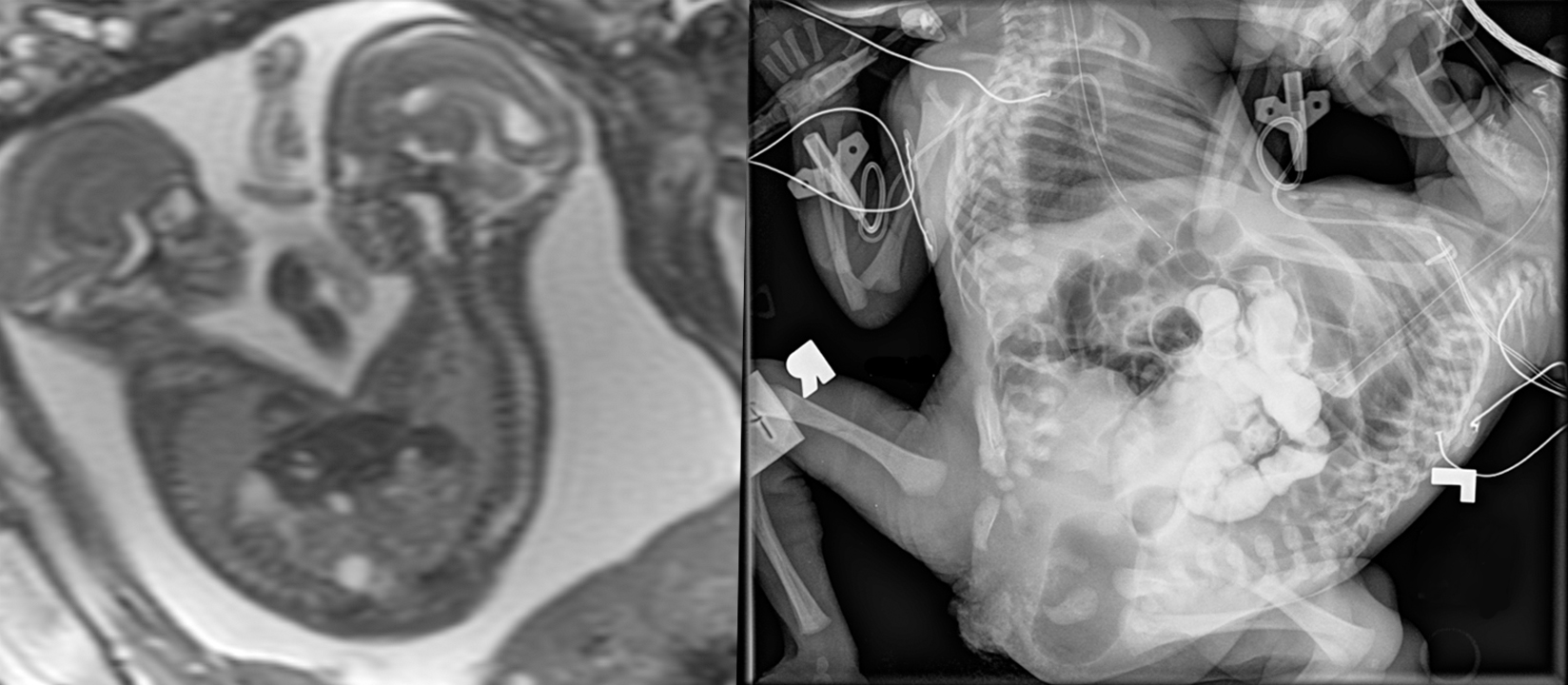
[Left]: Fetal MRI (FIESTA sequence) shows twins joined from their lower chest to the pelvis, but truly fused and sharing a single abnormal pelvic region. Not shown, but there are 3 lower limbs - one of the twins only had a single lower extremity.
[Right]: Postnatal small bowel follow-through (SBFT). It was unclear initially whether the twins shared a single rectum or had their own rectum. Therefore, contrast was administered via nasogastric tube for the twin with the suspected nonfunctional rectum, and serial imaging was performed until it passed into what turned out to be a separate, functional, but small rectum/anus.
I do not know too much about conjoined twins - not my area of expertise, but the general forms to consider are the side of fusion: ventral (front to front), lateral (side to side), dorsal (back to back), or caudal (tail end to tail end). Within these first 3, there are subtypes depending on how far up the fusion goes (head, chest, abdomen/pelvis); by definition, the caudal version obviously is only a lower body fusion. Once this is derived, an additional classification is the number of upper and lower limbs.
21
No clinical history saved on this one - sorry.
[Right] Small bowel follow-through (SBFT), where the patient drinks barium, and then we wait a bit until that barium is in the small bowel, then we take some pictures. This study is showing a long segment of terminal ileum that is strictured and severely narrowed in fibrostenotic Crohn's (red bracket). This is called the "string sign."
[Left] Coronal CT performed sometime after the SBFT. You can still see some residual barium in the small and large bowels (blue arrows). Red bracket shows the CT appearance of the terminal ileum stricture. On the CT, you can also see that the strictured segment has submucosal fat deposition, the "fat halo sign."
22
1
Two patients showing the varied appearance of large B-cell lymphoma of the stomach. [Gastrointestinal] [CT] [NM]
(lemmy.world)
I didn't save any clinical history for these - sorry.
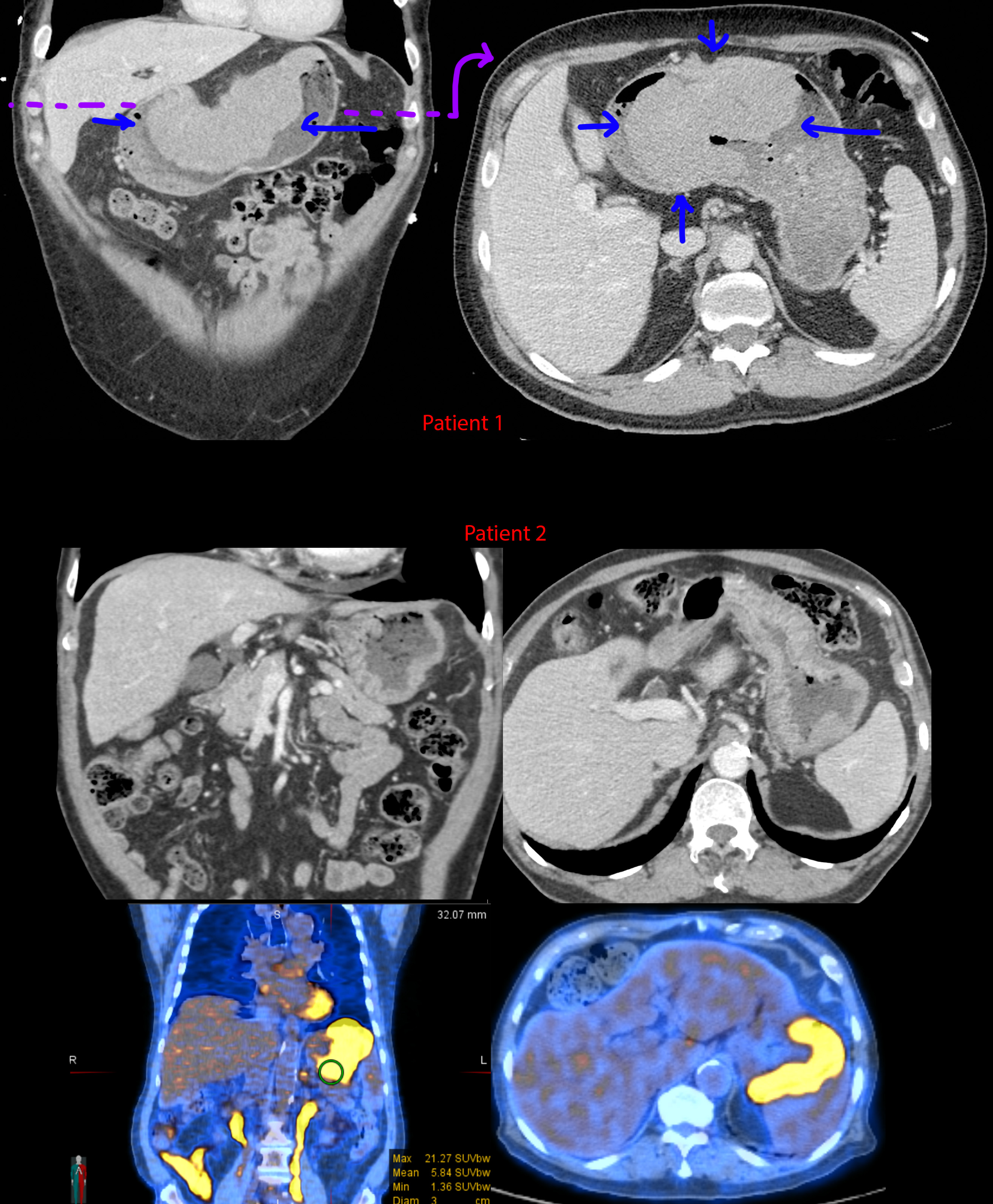
[Top] Patient 1 - Gigantic mass along the lesser curvature of the stomach. Look down at your belly - this mass is about 1/3rd the width from left to right.
[Mid] Patient 2 - CTs showing gently lobulated and undulating wall thickening of the gastric cardiac and fundus. Notice the transition from the normal gastric rugae to the smoother wall thickening where it is infiltrated by lymphoma. There is also mild (aneurysmal) dilation of the stomach where the wall thickening is located.
[Bottom] Patient 2 - PET-CT. The wall thickening is ridiculously hypermetabolic with a max SUV of 21.3. For comparison, the liver is normally in the range of 2-4 mean SUV.
Tuberculosis, sarcoidosis, lymphoma, and metastatic disease - these 4 can look like almost anything.
23
I can't tell much from this xray, but that shit hurt for awhile

25
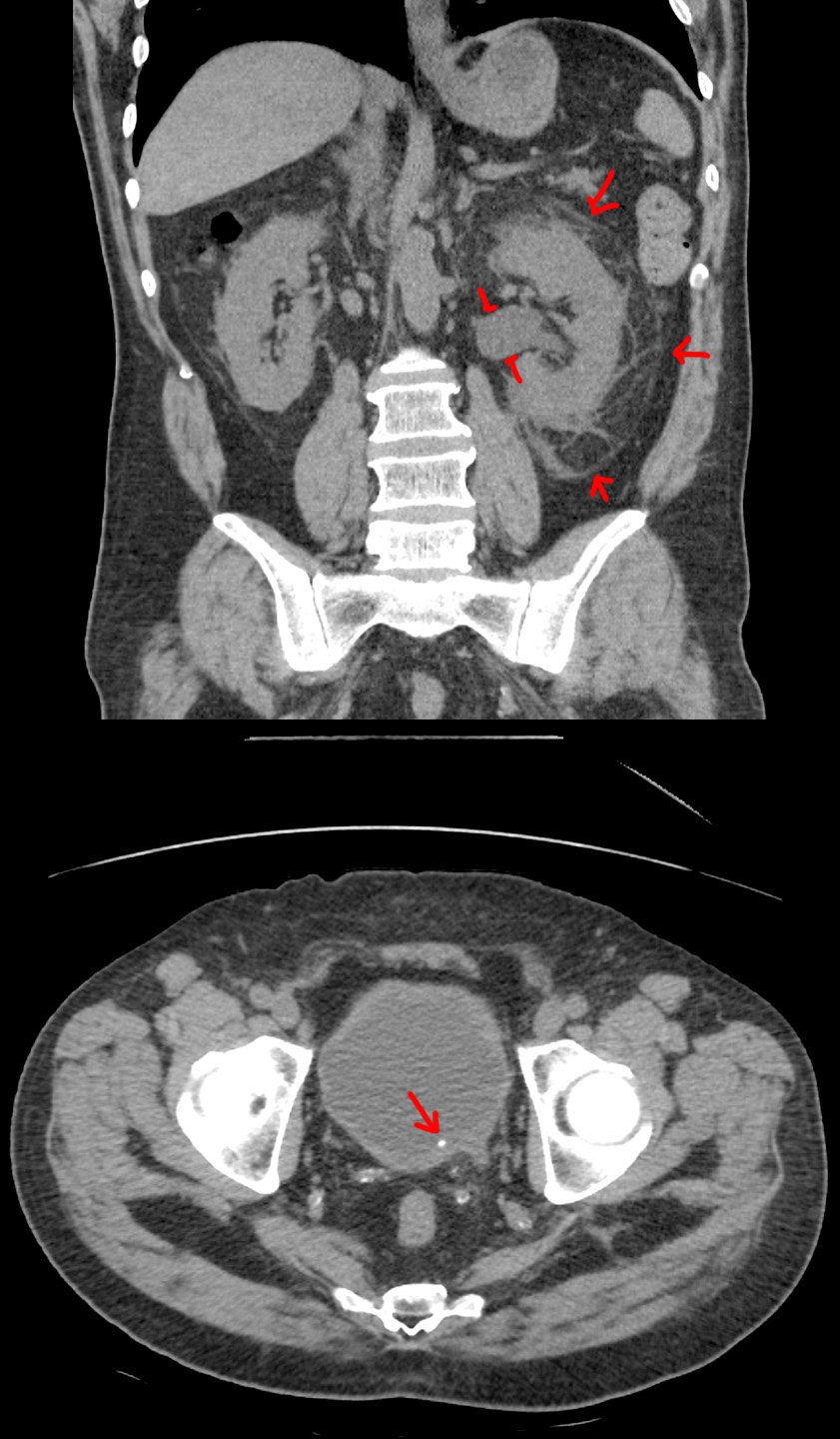
57 year old with left flank pain for 12 hours. Urine sample 2+ for blood. White count at 14.
[Top]: Coronal CT shows the left kidney is enlarged, with angry-looking, inflamed, surrounding fat. The renal pelvis is dilated (hydronephrosis).
[Bottom]: Axial CT shows a small stone at the very end of the ureter (ureterovesicular junction).
Pretty straightforward case. For the nonmedical visitors, this is what we look for if your doc wants to get a CT for flank pain / kidney stone suspicion. See the other case for an ultrasound version.
view more: next ›