26
25 year old with right flank and pelvic pain for 2 days. No fevers, chills, nausea, vomiting, or other urinary symptoms however.
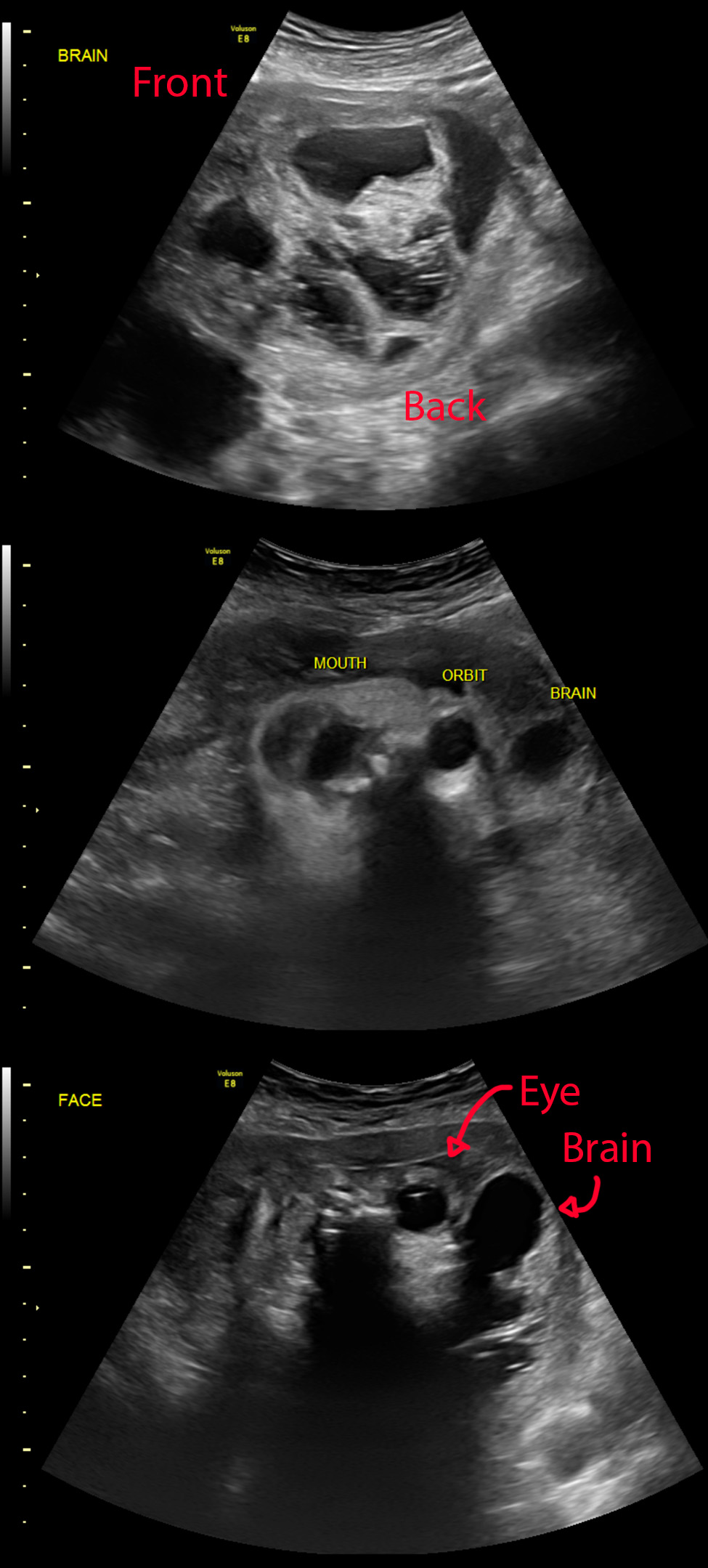
[Top]: Ultrasound shows right kidney with distended pelvis (hydronephrosis).
[Mid & Bottom]: Ultrasound transverse and sagittal images shows a 4.5 mm stone at the very end of the ureter (ureterovesicular junction).
Pretty straightforward case. For the nonmedical visitors, this is what we look for if your doc wants to get an US for flank pain / kidney stone suspicion. See the other case for a CT version.